
















5/19/2019
PITTSBURGH – Much like cancer, sepsis isn’t simply one condition but rather many conditions that could benefit from different treatments, according to the results of a University of Pittsburgh School of Medicine study involving more than 60,000 patients.
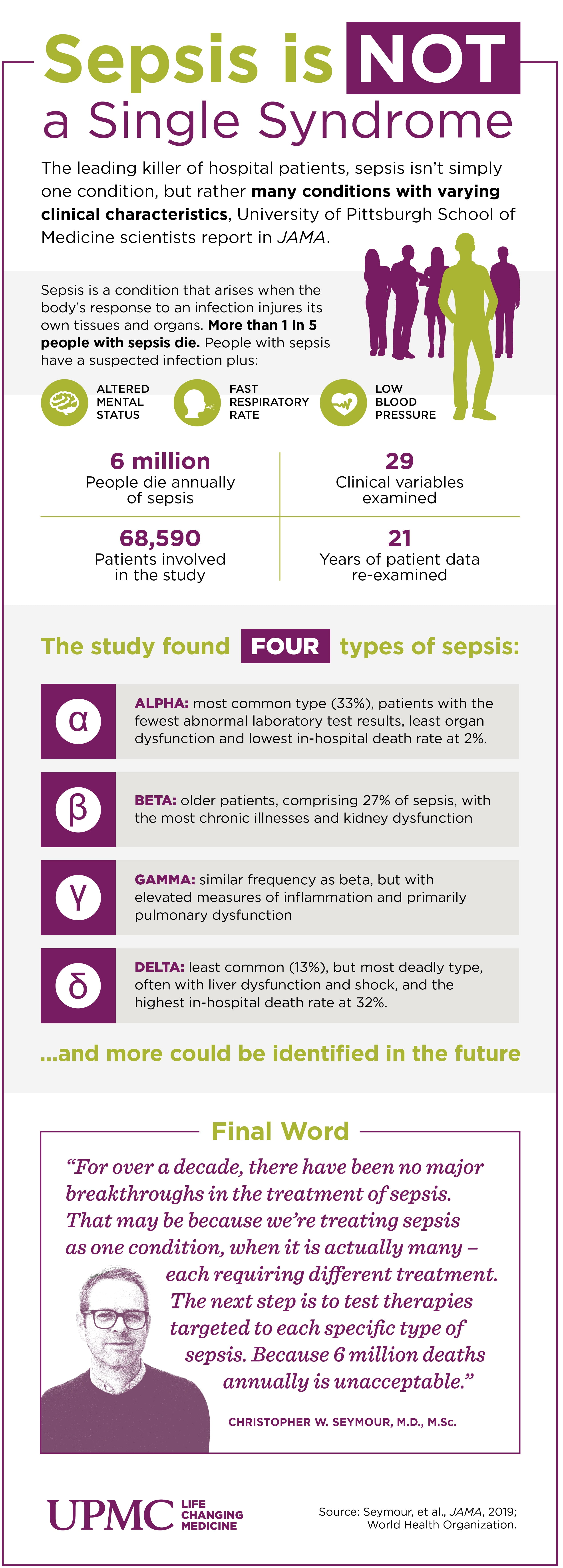
 “For over a decade, there have been no major breakthroughs in the treatment of sepsis; the largest improvements we’ve seen involve the enforcing of ‘one-size fits all’ protocols for prompt treatment,” said lead author Christopher Seymour, M.D., M.Sc., associate professor in Pitt’s Department of Critical Care Medicine and member of Pitt’s Clinical Research Investigation and Systems Modeling of Acute Illness Center. “But these protocols ignore that sepsis patients are not all the same. For a condition that kills more than 6 million people annually, that’s unacceptable. Hopefully, by seeing sepsis as several distinct conditions with varying clinical characteristics, we can discover and test therapies precisely tailored to the type of sepsis each patient has.”
“For over a decade, there have been no major breakthroughs in the treatment of sepsis; the largest improvements we’ve seen involve the enforcing of ‘one-size fits all’ protocols for prompt treatment,” said lead author Christopher Seymour, M.D., M.Sc., associate professor in Pitt’s Department of Critical Care Medicine and member of Pitt’s Clinical Research Investigation and Systems Modeling of Acute Illness Center. “But these protocols ignore that sepsis patients are not all the same. For a condition that kills more than 6 million people annually, that’s unacceptable. Hopefully, by seeing sepsis as several distinct conditions with varying clinical characteristics, we can discover and test therapies precisely tailored to the type of sepsis each patient has.”
 In the “Sepsis ENdotyping in Emergency Care” (SENECA) project, funded by the National Institutes of Health (NIH), Seymour and his team used computer algorithms to analyze 29 clinical variables found in the electronic health records of more than 20,000 UPMC patients recognized to have sepsis within six hours of hospital arrival from 2010 to 2012.
In the “Sepsis ENdotyping in Emergency Care” (SENECA) project, funded by the National Institutes of Health (NIH), Seymour and his team used computer algorithms to analyze 29 clinical variables found in the electronic health records of more than 20,000 UPMC patients recognized to have sepsis within six hours of hospital arrival from 2010 to 2012.
The algorithm clustered the patients into four distinct sepsis types, described as:
- Alpha: most common type (33%), patients with the fewest abnormal laboratory test results, least organ dysfunction and lowest in-hospital death rate at 2%;
- Beta: older patients, comprising 27%, with the most chronic illnesses and kidney dysfunction;
- Gamma: similar frequency as beta, but with elevated measures of inflammation and primarily pulmonary dysfunction;
- Delta: least common (13%), but most deadly type, often with liver dysfunction and shock, and the highest in-hospital death rate at 32%.
In the next part of the study, Seymour and his team applied their findings to several recently completed international clinical trials that tested different promising therapies for sepsis—all of which had ended with unremarkable results.
When trial participants were classified by the four sepsis types, some trials might not have been failures. For example, early goal-directed therapy (EGDT), an aggressive resuscitation protocol that includes placing a catheter to monitor blood pressure and oxygen levels, delivery of drugs, fluids and blood transfusions was found in 2014 to have no benefit following a five-year, $8.4 million study. But when Seymour’s team re-examined the results, they found that EGDT was beneficial for the Alpha type of sepsis patients. Conversely, it resulted in worse outcomes for the Delta subtype.
 “Intuitively, this makes sense—you wouldn’t give all breast cancer patients the same treatment. Some breast cancers are more invasive and must be treated aggressively. Some are positive or negative for different biomarkers and respond to different medications,” said senior author Derek Angus, M.D., M.P.H., professor and chair of Pitt’s Department of Critical Care Medicine. “The next step is to do the same for sepsis that we have for cancer—find therapies that apply to the specific types of sepsis and then design new clinical trials to test them.”
“Intuitively, this makes sense—you wouldn’t give all breast cancer patients the same treatment. Some breast cancers are more invasive and must be treated aggressively. Some are positive or negative for different biomarkers and respond to different medications,” said senior author Derek Angus, M.D., M.P.H., professor and chair of Pitt’s Department of Critical Care Medicine. “The next step is to do the same for sepsis that we have for cancer—find therapies that apply to the specific types of sepsis and then design new clinical trials to test them.”
Additional authors on this research publication are Jason N. Kennedy, M.S., Shu Wang, M.S., Chung-Chou H. Chang, Ph.D., Zhongying Xu, M.S., Gilles Clermont, M.D., M.Sc., Hernando Gomez, M.D., M.P.H., David Huang, M.D., John A. Kellum, M.D., Qi Mi, Ph.D., Victor Talisa, M.S., Shyam Visweswaran, M.D., Ph.D., Yoram Vodovotz, Ph.D., and Donald M. Yealy, M.D., all of Pitt; Corrine F. Elliott, M.S., and Scott Berry, Ph.D., both of Berry Consultants in Texas; Steven M. Opal, M.D., of Rhode Island Hospital; Tom van der Poll, M.D., Ph.D., of Pitt and the University of Amsterdam; Jeremy C. Weiss, M.D., Ph.D., of Carnegie Mellon University; and Sachin Yende, M.D., M.S., of Pitt and the VA Pittsburgh Healthcare System.
This research was funded by NIH grants R35GM119519, P50GM076659, R34GM102696, R01GM101197, GM107231, R01LM012095, K08GM117310-01A1 and GM61992.
MULTIMEDIA INFO: (click images for high-res versions and videos)
Top to Bottom:
Video caption: Dr. Christopher Seymour explains why sepsis is not just one disease and how we should treat it differently.
Credit: UPMC
Christopher Seymour, M.D., M.Sc., associate professor, University of Pittsburgh Department of Critical Care Medicine
Credit: University of Pittsburgh
Infographic caption: Sepsis is not a single syndrome, according to a University of Pittsburgh-led study in JAMA.
Credit: Chris Konopack/UPMC
Video caption: New findings from the University of Pittsburgh School of Medicine reveal that sepsis is not just one disease.
Credit: Speed Drawing Video
Derek Angus, M.D., M.P.H., professor and chair, University of Pittsburgh Department of Critical Care Medicine
Credit: University of Pittsburgh
